



Melt-off Body Fat With Economics & Common Sense
Summary
The widespread use of calorie restricted training (CRT) & calorie deficit training (CDT) on the onset of adopting a new lifestyle is providing success to small portions of the population but producing greater numbers of failure in the broader market. This means that we, as health professionals, are failing. That these approaches need to be revisited and reconsidered.
I believe that the vast majority of the US populace would be much better served by engaging in physical activity through a progression; establishing the routine, the understanding, and the proper techniques first. Gaining foundational education and routinizing and desensitizing the client with being present in a training environment, attaining comfortability in the space. All while maintaining what is a “normal” and healthy caloric intake for their individual bodily needs, preferably with shifts towards healthy food choices and an adherence to nutrient dense, bioavailable foods vs calorie dense food choices (i.e. whole foods vs fast foods). Smaller shifts allow for more consistent adherence, and establishment of routine with minimal introductions of environmental, behavioral, physiological and psychological stressors that CRT & CDT have been shown to introduce. Long-term adherence and small changes made over time provides consistency, a key marker in any measurement of success. Versus placing clients into CRT/CDT simply because they want to lose fat weight as fast as possible.
This essay aims to serve as my structured argument for why CRT & CDT are not strategies that are conducive to the rest-of-life success that so many are aiming for with a physical activity regimen as part of a lifestyle & body transformation roadmap. With a proposed strategy at the end of the paper.
The Common Path
What’s the common pathway for an individual first getting into the fitness space? Is it for health? Rarely. Is it for strength? Eh. Functional strength? Maybe. Is it to improve range of motion? Slightly more “maybe.” The most typical reason is to improve how one looks naked. This typically (due to the US population’s health demographics) involves an initial desire to “lose weight.” Or, what these individuals actually mean: “lose fat weight.” Maybe you’re one of these individuals. Maybe your goals involve a sliding scale between many, if not all, of the aforementioned motivations.


These individuals typically enter the gym space with a desire to see their abs again, or to slim down to fit into an old pair of pants, or to prepare for a wedding, or for bikini season — as it’s only a few weeks away. After spending all of the fall and winter months dragging their feet on getting started on the work. So these folks funnel into gyms and supplement stores looking for a get-fit-quick supplement & workout regimen — gotta make up for lost time.
What follows is a series of crossroads that get approached. They will either abandon their hopes & dreams for the sake of saving themselves the time & discomfort, or they decide to take a crack at it come hell or high water. At which point they go HAM (that’s “hard as a mother[expletive]” for those that don’t know) and drag themselves through absolute hell in an attempt to make up for that precious lost time. Some have the fortitude and willpower to make it happen; the abysmal “dieting” and forcing themselves to suffer through workouts for a predetermined length of time.
What follows is another crossroad; either they’ve achieved their short-term goal and then cease all activity that got them to their goal, or their goals adapt and shift. After seeing progress (if any) the adaptation in goals typically swings towards continuing the CRT/CDT agenda, or growing more muscle, or developing more strength (functional or otherwise).
What I aim to do here today is to elaborate on a few of the bases for where CRT/CDT theory originated, why conclusions from these origins are flawed, and why CRT and CDT should not be the first step in a body/lifestyle transformation plan.


Where did CDT come from as an approach to fat-weight loss? I have been attempting to pin it down but I cannot find a concrete source (if you do know, or know of a possibility that isn’t stated here please mention the book or study in the comments). But what I have been able to find is below, largely based off two sources:
(1) Eugene Sandow seems to be the first individual to be lent credit to CDT and its usefulness to get “ripped” quick (Sandow is also credited with being the first bodybuilder). A problem with this is that there is a difference between “getting in shape,” growing muscle, getting strong, and getting “ripped.” The key differentiator here being: getting “ripped” entails the muscle growth has already been attained, at which point the “getting ripped” part is a matter of aggressively reducing fat & water weight in order to appear lean in a short amount of time. Bodybuilders go to great lengths to show off their muscular developments as best they can, like reducing salt and carbohydrate intake to reduce water retention and make sure that their skin is as thin and tight to their muscular frame as possible while still being able to function. This is one of my issues with the widely adopted deployment of CDT for the average individual. While the average Jane & Joe may have goals that reside within the bodybuilding style format, the majority are not competing, and should not be putting their bodies through such rigorous treatment when they are not intending to compete.
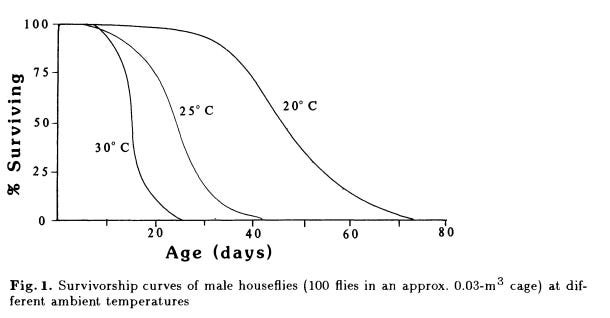
(2) is the “Rate of Living Theory” which was theorized by Max Rubner and interpreted by R.S. Sohal. Rubner claims that duration of life can be determined by the metabolic rate of an organism. Sohal tested this theory by keeping flies in environments of varying temperature and condition (being able to fly, or not) and observing the effects upon such things as metabolic rate and behavior (physical activity).

One of the major issues for me is that with Sohal’s study he found that the flies in the higher temperature environment lived shorter lives than those of cooler environments. The issue is that the conclusion was then made that the cause was the increased metabolic rate of the flies in the higher temperature, and not caused by the negative physiological effects that arise when an organism is introduced to an environmental temperature that exceeds their ideal neutral zone. Such as the diversion of nutrients and efforts towards mechanisms involved with the maintenance of internal body temperature homeostasis. Like reactions such as producing sweat when in a hot environment, or shivering when in a cold environment. Both require energy expenditure. Sohal’s study also does not give adherence to the effects of cortisol on resting energy expenditure (REE), as this study shows.
To Sohal’s credit, it was stated that the “Rate of Living Theory” likely cannot be equally applied across species, and even within specific species their are nuances that make it difficult to be applicable to populations. Therefore, this study’s findings within flies are likely irrelevant to the application of humans. Aside from some of the physiological mechanisms elaborated on, which we may have additional adaptive responses to balance out within our own physiologies. Ultimately what I am suggesting is that basing CDT/CRT on this theory is a lazy and irresponsible approach to justify these training/life styles.


The Body’s Responses To CRT & CDT
There has been very little discussion over how the body reacts to calorie restriction and how these adaptations can actually be negative for individual health, especially pertaining to the adaptations we aim to see when committing to body transformation. A narrative review published in May 2020 by Jasper Most and Leanne Marie Redman brought these points to light quite well.
“Reductions in energy expenditure (~5–10%) induced by 15–20% CR are reported consistently. Per ‘Rate of Living’-theory, this reduction attenuates the primary aging process and is therefore beneficial. The extent of this improvement is debatable. Previous studies have estimated that CR may increase lifespan by 5 years, if implemented early in adulthood, but only by 2 months, if implemented at age 60 (Most and Redman, 2017). These relatively small benefits in the elderly may be outweighed by the potential adverse effects of CR, e.g. reductions in metabolic rate and fat-free mass increase the risk for weight regain and frailty. CR may therefore not be an appropriate intervention for older individuals or those with relatively low fat-free mass.
“…The increased risk for weight regain, as demonstrated by different studies, may therefore relate to an insufficient adjustment of energy intake-regulating systems, which require further study. Investigating such systems including satiety and hunger sensation may also lead to strategies to facilitate long-term compliance to CR which is generally poor, and declines with the degree of CR prescription and duration of the intervention (Doucet et al., 2018).”
— Section 9 “Future directions”, Most & Redman (2020)
Most & Redman’s review laid bare the positives and negatives of CR as well as a decent attempt at discussing the benefits of combining CR with regular exercise with seemingly little-to-no bias.
The difficulty with arguing against CRT & CDT is that, with proper adherence to macro and micronutrients, baseline energy expenditure (EE) can tend to remain constant while energy intake (Calories) is extremely restricted (early on), resulting in adipose tissue reduction. That can be true. The problem is not that, the problem is that the general populace sees this result (the result that was desired) and then all discussion stops there. We got what we want, okay conversation: over. With very little (in my experience zero) discussion over the body’s adaptations to caloric restrictions and deficits, and the implications into the future.
For example, when you reduce the amount of energy you are taking in you therefore reduce the amount of energy available to consume (energy stored + energy ingested). Resulting in behavioral and physiological reductions in EE. Such as deciding to move less, be less active, engage in less cognitively taxing behavior because you’re “just too tired.” This was noted in the CALERIE trial, which is mentioned in both the Most & Redman study, quoted below, as well as here being referenced by Harvard.
“In CALERIE, a reduction in total daily EE and absolute activity-related EE was observed after 6 (Martin et al., 2011; Redman et al., 2009), 12 (Martin et al., 2011) and 24 months (Racette et al., 2017; Ravussin et al., 2015). After adjustment for the change in body mass, or sleeping metabolic rate, activity-related EE was still reduced after 6 months of CR. This suggests a lower level of physical activity, or a non-intentional “behavioral adaptation” thought to conserve energy (Redman et al., 2009).”
— Section 7 “Physical Activity”, Most & Redman (2020)
Showing that reductions in calorie consumption resulted in reduced activity even 2 years out. Being in a calorie deficit would likely only make the reductions in activity-related EE worse (assuming that the CR didn’t result in CD to begin with).
I don’t know about you, but my life tends to consistently demand more energy expenditure and investment…not less.
Another problem with CDT and it’s seeming basis from the “Rate of Living Theory” is that physical activity has been shown to increase longevity, as noted in this narrative review, in which regular physical activity (and the resulting body re-composition via improvements in strength and lean muscle mass) increase longevity alongside increasing resting metabolic rate. Going very contradictorily to the “Rate of Living Theory” on two counts; the longevity aspect as well as Rate of Living theory’s reducing of resting energy expenditure (REE) to increase longevity.
I would like to bring your attention to the following image, with focus being on the first paragraph in particular.

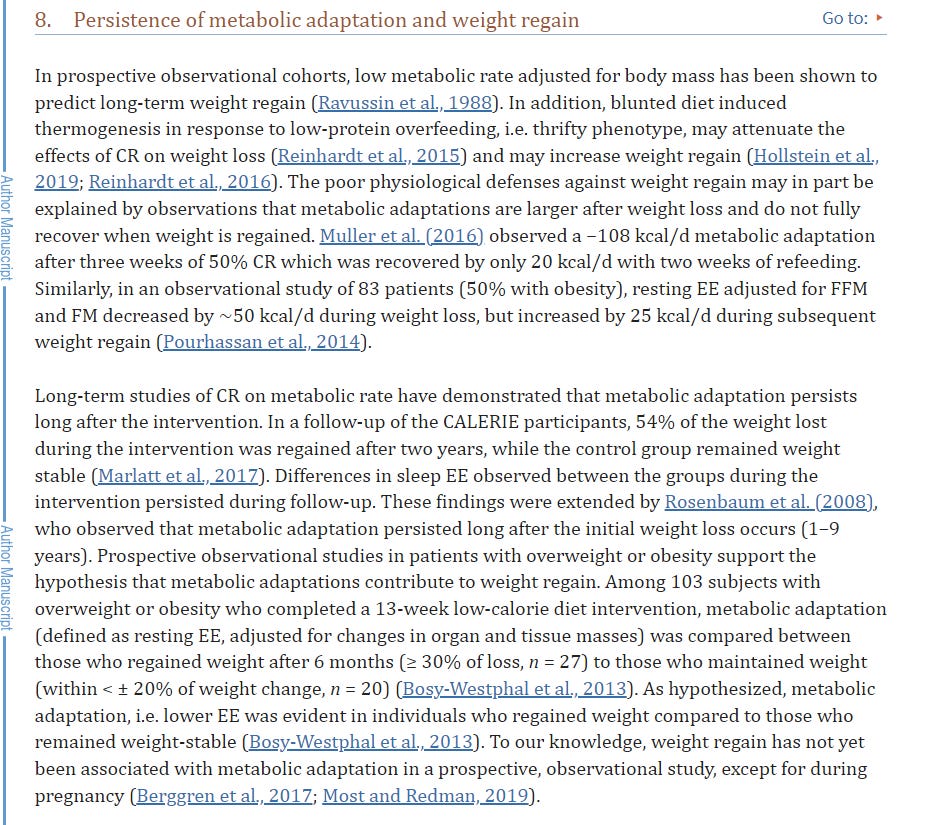
The above screengrab suggests in the first paragraph that the reduced metabolic rate adaptation from CR was maintained even after the weight was regained. Meaning that their resting metabolic rate (RMR) remained lower than before the CR strategy was adopted, even after the starting weight was returned to. Suggesting that it was now easier for the individual to gain weight than before, and they ended up right back at their starting weight. Placing them in a very net-negative position. Reducing RMR makes for less demand for calories, coupled with return to “normal” lifestyle and feeding habits, results in faster weight gain and weight retention.
The above paragraphs and the Most & Redman study corroborate my claims that CDT/CR are ultimately not long-term solutions to losing and keeping off fat weight, as well as being successful body transformation strategies.
Another Reason Why CDT & CRT Are Not Effective Strategies For Maintained Body Transformation
My biggest issue with CDT & CRT is that we are essentially providing conflicting stimuli to the body. Exercise is a growth stimulator, where as CR & CD are effectively growth limiters. When we engage in physical activity the aim is to provide stimuli that trigger adaptation responses (growing muscle, improving stroke volume of the heart, increasing metabolic rate, etc.). When the aim is in shrinking of the size of adipose tissue cells (yes they only shrink, the fat cells do not go away), or improving health & fitness, or life longevity, or all of the above, we essentially need the same outcome. That outcome is going to incorporate an accumulation of lean muscle mass, improvements in strength, as well as improvements in cardiovascular health markers. In order for these adaptations to take place the body must expend energy and resources in order to tweak our physiology to adapt to the stimuli we place upon our mortal shells.
By exercising in a calorie deficient state we are placing demands on our bodies without providing all of the required resources. The idea behind CDT is to provide all of these resources aside from calories, with the intent of forcing the body into providing the calories demanded via our fat stores. Which on its own triggers a metabolic rate reduction, while regular PA triggers a metabolic rate increase.
There’s also the psychological & emotional aspects to consider when putting an individual through caloric deficit; it’s stressful.
“In the presence of cortisol, muscle cells decrease glucose uptake and consumption and increase protein degradation; this supplies gluconeogenesis with glucogenic amino acids.[8] In adipose tissues, cortisol increases lipolysis. Lipolysis is a catabolic process that results in the release of glycerol and free fatty acids. These free fatty acids can be used in B oxidation and as an energy source for other cells as they continue to produce glucose. Lastly, cortisol acts on the pancreas to decrease insulin and increase glucagon.”
— Glucose and Protein Homeostasis; “Physiology, Cortisol” Thau, Ghandi, Sharma (2022)
The stress response in the body with the release of cortisol counteracts many of the responses we aim for with a body re-composition goal, and negatively impacts the recovery process. Running a risk of slowing down progress and potentially leading to heightened likelihood for injury or illness. This is why stress management is a key factor in any personal training or strength & conditioning regimen.
There’s also the matter to consider of how many of our clients are seeking to enact many of these lifestyle changes all at one time. Adopting an exercise routine coming from a sedentary lifestyle, “dieting,” entering a new environment that many deem to be intimidating, venturing into an area that many are uniformed in, being self-conscious of how they appear when in the gym, body dysmorphia… we can probably list even more friction-points. All of these can be stress-inducing for a client, and can therefore limit not only progress but adherence to a regimen. If a client engages in CDT for a few months and then relapses to their old ways, they run an increased risk of packing on more weight faster than before they started due to reductions in resting metabolic rate, cortisol exposure, dehydration, poor sleep, malnutrition, and so on.
My Proposed Shift In Approach
I propose a shift in the widely adopted strategy to body re-composition training. Instead of relying on CDT to give the client what they believe they want, I recommend a more educational approach to training. Contrary to the popularized phrase from the 90s and 2000s, the customer is not “always right.” Frankly, the customer is often even wrong, let alone misguided. The vast majority of the population knows that physical activity is healthy, but very few are informed on the reasons why. By this lens, to believe that these individuals could be right in the approach that is in their best interest just does not make any logical sense. The customer is very much free to seek out a trainer that confirms their bias(es), but it does not make them correct.
What I’m recommending is that trainers educate their clients on how their bodies actually work, before beginning training. Which will place pressure on many trainers but is absolutely necessary at our current juncture. As I am of the position that many, many trainers simply regurgitate what has been printed between the pages of textbooks without applying critical-thinking and original thought to these concepts and strategies.
I propose throwing CDT out the window for the majority of clients. CDT can play a more effective role in clients who need to lose weight rapidly for health reasons (such as the morbidly obese) or those that are preparing for a body composition competition like Mr. Olympia. But those individuals remain as outliers, for now.
Small Improvements + Consistency = Big Transformations
Once the routine is established, then, while still maintaining the same maintenance-level (or break-even) caloric intake, the client be engaged in either a hypertrophic or strength-aligned regimen. Grow the muscle underneath the adipose tissue. Increase bodily coordination and intero- & proprioception. Improve their understandings of how to use and move their bodies under the proper biomechanical forces and expressions of power. Growing the muscle without reducing the caloric intake will allow for the growth adaptations to occur more readily and even rapidly. While also providing proper instruction on the fact that delayed onset muscle soreness (DOMS) is not a required sensation for muscle growth. In fact, DOMS can often be misattributed with growth when in reality it can be signaling overtraining or undereating.


Taking an approach of making smaller, more committable improvements without immediately limiting caloric intake allows for the economics of the body to get where we want them with much less stress. Enabling the growth adaptations of muscle to occur will increase the baseline caloric demand of the body without restricting the caloric intake. Allowing for a much more smooth, and easy, and natural re-composition. Because eventually, as many of you may have guessed it, with this approach the baseline caloric demand can will) catch up to the caloric intake and achieve equilibrium.
At this point then the individual is free to engage in caloric restriction to induce fat loss if they would like, but this time instead they approach it with two major differences than if they started with CDT/CRT. First, the client has a foundation of muscle & strength that they would not have developed if they had started straight into CRT/CDT. Second, with that muscle they also have increased their baseline caloric demand before engaging in caloric restriction, meaning that the fat weight will quite literally melt off their bodies.
If the client were to be engaged in routines and strategies to maximize quality, routine sleep, with solid stress management in their lifestyles, coupled with healthy eating (not “dieting”) and hydration, their rates of success only increase.

